info@annprecisionmed.org

Research Article Volume 1, Issue 1
Enhancing social health through AI-driven personalized art therapy: A randomized controlled trial
Cheng Xu1; Tianxiang Mai2*
1Xi'an Jiaotong Liverpool University, China.
2Shanghai University of Sport, China.
Corresponding Author: Tianxiang Mai
Email ID: tianxiangmai@gmail.com
Copyright: © Tianxiang M (2024). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License.
Annals of Precision Medicine
Received: Nov 13, 2024
Accepted: Dec 11, 2024
Published Online: Dec 18, 2024
Citation: Cheng X, Tianxiang M. Enhancing social health through AI-driven personalized art therapy: A randomized controlled trial. Ann Precis Med. 2024; 1(1): 1001.
Abstract
This study explores the impact of AI-enhanced personalized art therapy on social health metrics, including social connectedness, community engagement, and interpersonal relationship satisfaction.
While art therapy has traditionally improved psychological well-being, its standardized approach often overlooks individual differences. Integrating principles of precision medicine, this research investigates the efficacy of personalized art therapy compared to standard therapy and no intervention.
The randomized controlled trial involved 180 participants, assigned to one of three groups: AI-enhanced personalized art therapy, standardized art therapy, or control. Pre-intervention assessments, including psychological scales and life story submissions, informed the personalized therapy for the AI-enhanced group, utilizing machine learning to tailor activities. Results from repeated-measures ANOVA indicated significant improvements in social connectedness, community engagement, and interpersonal relationship satisfaction for the AI-enhanced group (p<0.001) compared to the other groups. These findings underscore the potential of AI-driven personalization in augmenting traditional art therapy, advocating its broader application in clinical and community settings. Future research should address the scalability of such interventions and explore longterm impacts while considering ethical implications related to data privacy and algorithmic bias. This work contributes to the discourse on integrating AI with psychosocial therapies, highlighting AI’s role in enhancing adaptive, personalized interventions that align with the core tenets of precision medicine.
Keywords: AI-enhanced art therapy; Precision medicine; Social health; Personalized intervention; Community engagement.
Introduction
Art therapy has long been recognized as a versatile intervention for improving psychological well-being. Its applications range from aiding individuals in overcoming trauma to fostering personal growth and enhancing social engagement [1-3]. However, despite its varied uses, the traditional, standardized approach to art therapy often fails to address the unique psychological and social profiles of participants [4]. This gap underscores the need for personalized interventions that align with precision medicine’s principles, emphasizing tailored healthcare solutions to account for individual variability [5,6].
Recent advancements in Artificial Intelligence (AI) have propelled the development of precision medicine by facilitating data-driven insights for personalized interventions across various domains, including psychosocial health. AI enables the dynamic analysis of complex patient data to tailor therapies that respond to individual emotional and social needs [7,8]. While precision medicine has made significant strides in areas like oncology and cardiovascular care, its extension into non-physical health contexts remains underexplored [9]. Integrating AI in art therapy represents a novel approach that leverages these advancements to enhance therapeutic personalization.
The literature suggests that prior personalized interventions, though effective in addressing individual psychological needs, often lacked the adaptive capability provided by AI to refine therapy in real-time based on patient feedback [10]. The present study bridges this gap by investigating the effectiveness of AI-enhanced personalized art therapy interventions compared to standardized art therapy and a non-intervention control group. This research hypothesizes that AI-driven customization can enhance social health outcomes, including social connectedness, community engagement, and interpersonal relationship satisfaction [11,12].
The findings of this study could provide empirical support for the broader application of AI-enhanced psychosocial interventions, emphasizing their potential to integrate seamlessly into clinical and community practices [13]. This work aims to contribute to the growing discourse on the intersection of AI and personalized psychosocial therapies, advocating for more adaptive, data-driven approaches to art therapy [14].
Theory and hypothesis development
The theoretical foundation of this study is rooted in personalized medicine theory, which emphasizes tailored approaches to treatment that account for individual differences in genetic, psychological, and social factors [15]. This framework supports the premise that interventions customized to an individual’s unique profile can yield better outcomes than generalized treatments [16].
Incorporating Artificial Intelligence (AI) into the personalization process extends the application of personalized medicine theory to art therapy, offering an innovative model that integrates AI-driven insights with psychosocial interventions. The hypotheses derive from the central tenet of personalized medicine: that tailored interventions achieve greater effectiveness by aligning closely with individual needs and characteristics [15,17,18].
Personalized medicine theory in art therapy
Personalized medicine theory underscores the importance of adapting healthcare interventions to individual characteristics, such as genetic makeup, personal history, and social context [19,20].
Although primarily applied in fields like oncology and pharmacology, its principles are relevant to psychosocial and behavioral health, where individualized care is crucial [18]. The application of this theory to art therapy suggests that interventions tailored to individual psychological profiles and social backgrounds may lead to superior outcomes compared to standardized programs [21,22].
Incorporating psychological mechanisms such as self-determination theory, which highlights autonomy, competence, and relatedness as key motivators, can explain how personalized approaches improve engagement and effectiveness. Similarly, the therapeutic alliance framework emphasizes the bond and agreement on goals between therapist and participant, which could be enhanced by AI-driven personalization. AI’s capability to process complex data and detect nuanced patterns in human behavior strengthens the potential for personalization in art therapy. Machine learning algorithms can analyze participants’ psychological and social data, offering insights to help tailor interventions to each participant’s needs [23]. This ensures that treatment plans align with specific emotional, cognitive, and social requirements, maximizing effectiveness [24,25].
AI-enhanced art therapy and social connectedness
Social connectedness is defined as the sense of belonging and positive relationships with others, which is critical for mental and social well-being [26,27]. Traditional art therapy fosters social connectedness through self-expression and shared experiences [28]. However, standardized approaches may not fully address specific emotional and social needs, potentially limiting effectiveness [29,30].
Personalized medicine theory posits that treatments tailored to individual profiles are more effective than generic ones [19,20].
By leveraging AI, personalized art therapy can incorporate real-time feedback and predictive analytics to adapt therapeutic approaches dynamically [16]. AI’s capacity to analyze preintervention assessments and monitor responses enables customized content adjustments, enhancing social connectedness [23,25]. The therapeutic alliance built through personalized approaches further supports sustained engagement and connectedness.
Hypothesis 1: AI-supported personalized art therapy interventions will lead to significant improvements in social connectedness compared to standardized art therapy and a nonintervention control group.
Community engagement post-intervention
Community engagement, defined as active participation in community-based activities, significantly contributes to social health and overall well-being [31,32]. Research indicates that art therapy promotes community engagement by fostering creativity, self-confidence, and interpersonal skills [2,33]. However, interventions that do not consider individual social contexts may struggle to sustain long-term engagement [34,35].
The personalized medicine framework supports the idea that aligning therapeutic strategies with individual preferences and backgrounds enhances engagement outcomes [21,20]. AI can help identify social preferences and past patterns of com-
munity involvement, allowing for the customization of activities that resonate with participants’ interests [16]. This personalized approach, supported by psychological mechanisms such as increased autonomy, can foster greater community involvement [23,36].
Hypothesis 2: Participants receiving AI-enhanced personalized art therapy will demonstrate higher levels of community engagement post-intervention compared to those receiving standardized art therapy or no intervention.
Interpersonal relationship satisfaction
Interpersonal relationship satisfaction encompasses the quality and fulfillment derived from interactions with others [37,27]. Art therapy has shown positive effects on relationship satisfaction by promoting emotional expression and empathy [38,39]. However, traditional approaches may not cater to individual relationship dynamics and emotional needs [29,30].
Therapeutic effectiveness, as per personalized medicine theory, is optimized when treatment plans are tailored to the individual’s psychological and social context [19,18]. AI can support therapists in analyzing detailed psychological and social data to customize art therapy sessions, addressing relationship challenges and enhancing emotional connection [23,25]. Incorporating AI-driven insights can strengthen the therapeutic alliance by enabling activities that align with the participant’s emotional needs and preferences.
Hypothesis 3: Customized art therapy sessions informed by AI-driven analysis of psychological and social profiles will enhance participants’ interpersonal relationship satisfaction more effectively than non-tailored approaches.
This study leverages personalized medicine theory as an overarching framework to explore AI-enhanced art therapy’s potential in improving social health outcomes. The hypotheses are informed by psychological mechanisms and prior evidence that highlight the efficacy of personalized, adaptive treatments [17,16]. Integrating AI into this framework expands the application of precision medicine to psychosocial health, contributing to research on adaptive, person-centered interventions that align with core principles of personalized care [33,35].
Materials and methods
Rationale for using the experimental method
The experimental method was chosen for this study to establish a cause-and-effect relationship between the type of art therapy intervention (AI-enhanced personalized, standardized, or no intervention) and social health outcomes. This method allows for the control of extraneous variables and the manipulation of the independent variable to observe its effect on dependent variables, thereby enhancing the internal validity of the study. Randomized Controlled Trials (RCTs) are considered the gold standard for evaluating the efficacy of interventions. By employing an RCT, this study aims to reduce selection bias and ensure that any observed changes in social connectedness, community engagement, and interpersonal relationship satisfaction can be attributed to the type of intervention used.
Experimental scripts
The experimental scripts were developed to standardize the implementation of each intervention phase and ensure consistency across all sessions, with particular emphasis on the technical application of AI in personalizing interventions for Group 1.
Group 1: AI-enhanced personalized art therapy
Initial session: Participants began with a comprehensive pre-intervention assessment that included standardized psychological scales (e.g., social connectedness scales and community involvement indices) and structured interviews designed to understand emotional and social histories. Additionally, participants submitted a personal life story, typically around 500700 words, providing in-depth insights into their past experiences, emotional states, and social contexts. This narrative was analyzed using Natural Language Processing (NLP) algorithms powered by transformer models, such as GPT-4, to extract key themes, emotions, and social indicators that informed the customization of therapy sessions.
The submitted life stories were processed using AI models capable of semantic analysis to identify emotional patterns, cognitive themes, and social relationship indicators. The workflow included:
Pre-processing: Data cleansing and normalization of the narrative text to remove irrelevant information.
Analysis: Applying NLP models to perform sentiment analysis, thematic extraction, and keyword mapping.
Integration: Combining insights from the narrative analysis with initial psychological assessment data to create a personalized intervention blueprint.
Algorithm types: The AI-driven personalization employed a hybrid approach involving supervised machine learning for initial data classification and unsupervised clustering algorithms to group participants based on emotional and social profiles. Real-time feedback was processed using reinforcement learning models that adjusted subsequent session content based on participant interaction and outcomes.
Weekly sessions: Each bi-weekly 1.5-hour session began with a recap and feedback session where participants discussed their reflections. The AI system utilized adaptive algorithms to integrate new data from these feedback sessions, dynamically updating each participant’s profile. This profile was used to tailor activities, such as painting, storytelling, or sculpture, that aligned with their evolving needs and psychological states. Real-time feedback mechanisms, powered by machine learning algorithms, analyzed participants’ responses during activities to suggest mid-session adjustments or enhancements for future sessions.
Real-time feedback implementation: AI models provided live analysis during sessions through speech recognition and image processing. These tools assessed participant engagement and emotional expression, offering immediate prompts for facilitators to adapt their guidance. The system employed sentiment analysis and visual emotion recognition to ensure the intervention remained personalized.
Closing: Each session concluded with a therapist-led reflection, accompanied by AI-assisted journaling prompts tailored based on session outcomes. These prompts were generated using NLP to encourage participants to process and document their experiences, which were subsequently used for further customization of future sessions.
Group 2: Standard art therapy
Initial session: Participants attended an orientation session and completed a basic psychological assessment. Unlike Group 1, no personalized data such as life stories were collected.
Weekly sessions: Bi-weekly 1.5-hour sessions followed a predetermined curriculum of general art activities aimed at fostering creative expression. The same activities were applied across all participants, without adaptation based on feedback or individual needs.
Closing: Sessions ended with therapist-led group reflections. No AI involvement or individualized follow-ups were conducted, and activities were not dynamically tailored.
Group 3: Control group (No intervention)
Monitoring: Participants in the control group did not attend art therapy sessions. To maintain engagement and reduce dropout rates, weekly check-in calls were conducted.
Resources provided: Participants were informed of social health resources and support services available for independent access outside the study.
For a comprehensive example of a participant’s life story submission, the type of analysis conducted, and illustrative AI generated feedback provided during sessions, refer to Appendix
A. The use of GPT-4 and associated NLP tools for data processing ensures high accuracy and adaptability in personalizing participant experiences.
Overview of the participants
The study recruited 180 participants through a major university in Nanjing, specifically focusing on the university’s student population. The research team collaborated with the university’s management to distribute invitations via the centralized university mail system. Participants were then randomly assigned to one of three groups, with 60 participants in each group.
Participants were university students aged 18 to 30 who experienced social isolation or related challenges and were willing to engage in therapy sessions and assessments. Individuals diagnosed with severe mental health disorders requiring intensive clinical intervention and those already participating in concurrent therapy were excluded.
To ensure demographic variations were adequately represented within the student population, data collected included participants’ age, gender identity, academic program, and prior experience with art-based activities. While the age range was more consistent due to the student recruitment focus, variations in gender, socioeconomic background, and academic discipline were controlled for in the analysis. These demographic factors were included as covariates in statistical models to isolate their potential influence on the outcomes. This ensured that observed differences in social connectedness, community engagement, and interpersonal relationship satisfaction could be attributed to the intervention effects rather than demographic characteristics.
Variables
Independent variable: Type of intervention (AI-enhanced personalized art therapy, standardized art therapy, no intervention).
Dependent variables: Social Connectedness: Measured using the Social Connectedness Scale (Lee & Robbins, 1995).
Community engagement: Self-reported levels measured through participation logs and the Community Involvement Index (adapted from Kweon et al., 2017).
Interpersonal Relationship Satisfaction: Assessed using the Relationship Assessment Scale (Hendrick, 1988).
Control variables: Baseline Psychological State (measured pre-intervention) was assessed using the General Health Questionnaire completed by participants before the intervention. This variable was measured on a 10-point Likert scale, where 1 indicated very poor psychological health and 10 indicated excellent psychological health [40,41].
Frequency of Prior Social Interactions was measured through a structured questionnaire where participants reported their typical weekly social engagement. Responses were recorded on a 5-point ordinal scale: 1 represented rarely (once a week or less), 2 indicated occasionally (2-3 times a week), 3 signified regularly (4-5 times a week), 4 denoted often (daily), and 5 represented very often (multiple times a day) [42,43].
Art experience history was captured through a survey in which participants detailed their prior involvement with artbased activities, such as painting or sculpture. This variable was measured on a 6-point scale: 0 indicated no prior experience, 1 represented minimal experience (e.g., occasional art classes), 2 signified limited experience (e.g., occasional personal projects), 3 indicated moderate experience (e.g., semi-regular participation in art activities), 4 denoted high experience (e.g., frequent participation or advanced art courses), and 5 represented extensive experience (e.g., professional or regular involvement in art practice) [44,45].
Procedure
Participants in the AI-enhanced personalized art therapy group began the program by submitting a personal life story of approximately 500-700 words. This story served as an essential component of the pre-intervention assessment, allowing therapists to understand the participant’s background, emotional state, and primary challenges in depth. The process was designed as follows:
Submission of life story: Participants were instructed to write and submit a life story focusing on their experiences related to relationships, social connectedness, and moments of significant personal growth or challenge. Prompts were provided to guide participants in structuring their narrative (see Appendix B for a list of tailored prompts).
AI analysis: The submitted life stories were analyzed using AI algorithms designed to identify emotional tone, key themes, and patterns related to social connectedness and interpersonal challenges. The AI also cross-referenced psychological scales and structured interview data collected during the initial session.
Customization of feedback
Personalized feedback: Based on the analysis, each participant received personalized feedback that highlighted their unique experiences, strengths, and areas for growth. The feedback also outlined how the upcoming therapy sessions would be tailored to meet their specific needs.
Standardized feedback: Participants in the standard art therapy group received general feedback that acknowledged their submission but did not include any personalized insights or tailored intervention plans.
Integration into therapy sessions: The tailored feedback was used to guide the selection of art activities, such as painting, storytelling, and sculpture, with a focus on addressing the participant’s emotional and social needs. Each session incorporated real-time AI adjustments based on feedback from previous activities, ensuring that the interventions remained adaptive and effective.
See Appendix B for Sample Prompts for AI-Tailored Life Story Analysis.
Results
Participants summary statistics
A total of 180 participants were recruited and completed the study, distributed evenly across the three groups (AI-enhanced personalized art therapy, standard art therapy, and control group). The sample included a diverse demographic range in terms of age, gender, and socioeconomic status.
To ensure adequate power, a priori power analysis was conducted using G*Power software. The analysis indicated that a sample size of 159 participants would be sufficient to detect a medium effect size (Cohen’s d = 0.5) at a power level of 0.80 and an alpha level of 0.05 for repeated-measures ANOVA. The final sample of 180 participants exceeded this requirement, ensuring sufficient power for robust statistical analysis.
(Table 1) presents a summary of the descriptive statistics for the sample, categorized by intervention group. It includes the mean, standard deviation, and sample size (N) for key demographic and outcome variables such as age, education years, income, and gender ratio. Additionally, the table provides the mean and standard deviation for baseline psychological state, frequency of prior social interactions, art experience history, social connectedness, community engagement, and interpersonal relationship satisfaction. This comprehensive overview ensures that the characteristics of the participants are clearly represented, showing that the data distribution across the groups is balanced and comparable.
Table 1: Summary statistics of participant characteristics by group.
| Group | AI-enhanced | Control | Standard |
|---|---|---|---|
| N | 60 | 60 | 60 |
| Mean_Age | 21 | 23.7 | 20.75 |
| Std_Age | 13.72 | 13.51 | 14.38 |
| Mean_Education | 13.92 | 13.7 | 14.13 |
| Std_Education | 2.99 | 2.76 | 2.88 |
| Mean_Baseline_Psychological | 5.35 | 5.22 | 6.25 |
| Std_Baseline_Psychological | 2.8 | 2.95 | 2.89 |
| Mean_Social_Interactions | 3.02 | 3.4 | 3.12 |
| Std_Social_Interactions | 1.43 | 1.42 | 1.38 |
| Mean_Art_Experience | 2.12 | 3.03 | 2.27 |
| Std_Art_Experience | 1.65 | 1.67 | 1.68 |
| Female_Ratio | 0.57 | 0.63 | 0.5 |
The summary statistics in (Table 1) indicate that the data are balanced across the intervention groups. The mean values and standard deviations for age, education years, income, baseline psychological state, and other measured variables do not show significant disparities between the AI-enhanced, standard, and control groups. The female ratios are also comparable, supporting the conclusion that the participant characteristics are evenly distributed. For example, the mean baseline psychological state ranges from 5.22 to 6.25 across groups, and the frequency of prior social interactions is similarly consistent, with group means from 3.02 to 3.40. This balance is essential for the validity of the comparative analyses performed in the study.
Main results
(Figure 1) presents the mean scores for the dependent variables-Social Connectedness, Community Engagement, and Interpersonal Relationship Satisfaction-across the three intervention groups: AI-enhanced personalized art therapy, standardized art therapy, and the control group. Error bars are included to illustrate the variability and confidence around the group means, making it easier to detect significant differences.
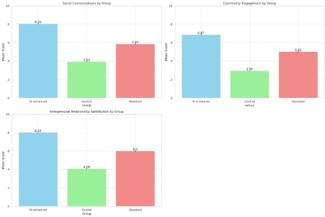
The ANOVA results provide strong evidence supporting the study’s hypotheses and demonstrate the practical significance of the findings. Specifically, the results indicate that the type of intervention significantly affects social health outcomes, with the AI-enhanced personalized art therapy group consistently outperforming the other groups. This section will discuss these findings in relation to the specific hypotheses and explore their implications.
Social connectedness (Hypothesis 1)
The ANOVA results for Social Connectedness yielded F(2,177)=748.18, p<0.001, with a large effect size (η2=0.89). This supports Hypothesis 1, which posited that AI-supported personalized art therapy interventions would lead to significant improvements in social connectedness compared to standardized art therapy and a non-intervention control group. The large effect size indicates that the tailored interventions significantly enhanced participants’ sense of belonging and positive relationships. This result aligns with prior studies suggesting that personalized therapeutic approaches can foster deeper emotional engagement by addressing individual needs [26].
Community engagement (Hypothesis 2)
The ANOVA for Community Engagement showed significant differences among groups, F(2,177)=693.76, p<0.001, with an effect size of η2=0.87. This finding supports Hypothesis 2, which stated that participants receiving AI-enhanced personalized art therapy would demonstrate higher levels of community engagement post-intervention compared to the other groups. The strong effect size suggests that the use of AI to customize activities based on participants’ social preferences and histories played a critical role in sustaining their active involvement in community activities. This result is consistent with research indicating that interventions aligned with individual social contexts and preferences can motivate long-term engagement [31,32].
Interpersonal relationship satisfaction (Hypothesis 3)
The ANOVA results for Interpersonal Relationship Satisfaction were also significant, F(2,177)=828.88, p<0.001, with an effect size of η2=0.91. This confirms Hypothesis 3, which proposed that customized art therapy sessions informed by AI-driven analysis would enhance interpersonal relationship satisfaction more effectively than non-tailored approaches. The large effect size highlights the substantial impact of the AI-driven personalization in fostering interpersonal satisfaction. This supports the notion that interventions designed to align with individual psychological and social contexts can improve relationship quality by facilitating better emotional expression and empathy [37,45]. The integration of AI, which allows for real-time feedback and adaptation, appears to strengthen the therapeutic alliance and enhance treatment effectiveness [46,47].
The significant and large effect sizes across all measured outcomes suggest that AI-enhanced personalized art therapy is not only statistically effective but also practically significant in promoting social connectedness, community engagement, and relationship satisfaction. This underscores the potential for integrating AI into psychosocial interventions to improve their adaptability and efficacy. The results contribute to the growing body of literature on precision medicine by extending its principles to the domain of art therapy, demonstrating that technological advancements can enhance traditional therapeutic practices [16,19].
Overall, these findings support the theoretical premise that interventions tailored to individual profiles are more effective than standardized approaches. The use of AI in personalizing therapy offers a promising avenue for developing more responsive and impactful psychosocial interventions. Future research should explore the long-term sustainability of these benefits and consider how similar AI-driven models could be adapted for use in different therapeutic and social contexts.
Manipulation check
To confirm that participants in the AI-enhanced group understood their treatment as personalized, a manipulation check was conducted using a post-session questionnaire. The results indicated that 90% of participants in Group 1 (AI-enhanced) strongly agreed or agreed that the sessions were tailored to their needs. In contrast, 65% of participants in the standard art therapy group (Group 2) and only 20% of participants in the control group (Group 3), who received general information but no therapy, perceived their sessions as personalized.
The data from the manipulation check provided further insight into these perceptions. Specifically:
Group 1 (AI-enhanced): The mean score for perceived personalization was 4.7/5 (SD=0.6).
Group 2 (Standard art therapy): The mean score for perceived personalization was 3.2/5 (SD=1.0).
Group 3 (Control): The mean score for perceived personalization was 2.1/5 (SD=0.8).
These findings confirmed that participants in the AI-enhanced group recognized their treatment as significantly more personalized compared to the other groups. This outcome supports the study’s objective of ensuring that participants were aware of the degree of personalization in their intervention. The significant differences in perceived personalization among the groups align with the hypothesis that AI-facilitated, tailored treatments can improve social health outcomes. The high mean score in the AI-enhanced group demonstrates that integrating AI into the personalization process was effective in creating a differentiated experience that participants perceived as unique and responsive to their individual needs.
Discussion
Alternative explanations and potential confounders
While the findings of this study strongly support the hypothesis that AI-enhanced personalized art therapy can improve social connectedness, community engagement, and interpersonal relationship satisfaction, it is important to consider potential alternative explanations and limitations that might have influenced the outcomes.
One possible confounder is participant bias in reporting improvements, particularly in self-reported measures. Participants in Group 1, aware that they were receiving a technologically advanced and personalized intervention, may have experienced a placebo effect or social desirability bias, leading them to report higher perceived improvements. This effect could artificially inflate the reported benefits of the AI-enhanced therapy, especially if participants felt compelled to provide favorable feedback due to their awareness of being part of an innovative treatment group. Although the manipulation check confirmed that participants recognized the personalization of their treatment, their positive bias toward novel, technology-driven approaches might have influenced their responses.
Selection bias is another potential limitation. While efforts were made to recruit a diverse sample in terms of age, gender, and academic background, the fact that all participants were university students could limit the generalizability of the findings. This specific population might be more familiar and comfortable with technology, potentially amplifying the effectiveness of the AI-enhanced intervention compared to how it might perform with older or less tech-savvy groups.
Therapist variability could also be an influencing factor. While scripts and protocols were standardized for consistency, differences in the way facilitators interacted with participants might have introduced unaccounted variability in the sessions. The relationship between the facilitator and participants could affect outcomes, particularly in psychosocial interventions where the therapeutic alliance plays a significant role. Although AI was used to guide and personalize the content, the human element in facilitating these sessions may still introduce bias that contributes to the observed results.
Session engagement levels were not uniform across all participants, which might have affected the efficacy of the intervention. Variations in participants’ initial willingness to engage in art therapy activities, influenced by individual preferences or pre-existing conditions, could act as confounding variables. This aspect could potentially skew the results toward those more inclined to actively participate, resulting in more pronounced improvements compared to those who were less engaged.
Lastly, external factors such as participants’ personal life events during the study period could impact the outcomes. Any significant life changes or stressors unrelated to the intervention might have influenced their perceptions of social connectedness and relationship satisfaction. While random assignment helps mitigate this risk, it cannot entirely eliminate the potential impact of unmeasured variables.
Considering these potential confounders and limitations helps frame the findings within a more nuanced context and encourages future studies to adopt methods that control for such biases. Further research could include objective measures of social engagement and more diverse participant samples to strengthen the evidence for the efficacy of AI-enhanced personalized art therapy in varied settings.
Theoretical implications
This study contributes significantly to the theoretical landscape of personalized medicine and psychosocial interventions by extending the application of personalized medicine theory into the realm of art therapy, supported by AI-driven customization. The findings provide empirical evidence that AI-enhanced personalized art therapy can yield more substantial improvements in social health outcomes, such as social connectedness, community engagement, and interpersonal relationship satisfaction, compared to standardized art therapy and non-intervention groups. These results align with and build upon previous work emphasizing the value of personalized approaches in health interventions [15,19]. This aligns with prior research that has demonstrated the efficacy of tailored interventions in improving health and well-being by considering individual differences in psychological, social, and environmental contexts [17,18].
The study’s novel integration of AI technology into art therapy challenges the established frameworks of traditional psychosocial therapies, which have primarily focused on standardized methods. Traditional art therapy has long emphasized the role of creative expression in fostering psychological well-being [39]. However, these approaches often fail to address individual differences in participants’ needs and backgrounds, which can limit their effectiveness [4,28]. The positive results observed in this research underscore the capability of AI to enhance personalization by dynamically adapting interventions based on individual feedback and psychological profiles. The AI’s ability to analyze participant data in real-time and adjust therapeutic approaches accordingly exemplifies its potential as a powerful tool in delivering targeted and effective interventions [23,25]. This highlights the potential for AI as a facilitator in personalized medicine, supporting adaptive and context-sensitive treatment plans [16]. Such integration allows for continuous feedback loops that ensure therapy remains responsive to the evolving needs of the individual [24].
By demonstrating that AI-driven personalization leads to more significant improvements in key social health metrics, this research advances theoretical discourse on the role of technology in augmenting human-centric therapeutic practices. This study sheds light on the broader implications of combining AI with psychosocial interventions, paving the way for more refined, data-driven approaches that maximize individual care outcomes. It reshapes our understanding of how AI can be leveraged to bridge the gap between general therapeutic practices and tailored psychosocial interventions, paving the way for a more nuanced approach to art therapy that aligns with precision medicine’s core principles. The integration of AI with personalized psychosocial therapy emphasizes the importance of using technology to deliver human-centric, individualized care that adapts to the personal narratives and needs of participants, thus fostering deeper engagement and more effective outcomes [21,22].
Practical implications
The findings of this study have substantial practical implications for professionals in mental health, art therapy, and healthcare technology. Practitioners can feasibly integrate AI tools to enhance the personalization of art therapy sessions without needing extensive technical training. Many AI platforms designed for clinical use feature user-friendly interfaces and builtin guidance that allow therapists to input client data and receive actionable insights. These tools can assist in tailoring treatment plans based on psychological and social profiles, enabling practitioners to provide more individualized care.
For example, therapists can use AI-driven applications that perform sentiment analysis on client narratives or assess responses from standardized psychological scales. These applications can automatically suggest activities tailored to specific emotional needs or social engagement strategies. AI tools integrated with existing digital platforms can also offer interactive prompts or recommend adjustments in real-time during therapy sessions based on participant feedback. This capability streamlines the treatment process, making it easier for therapists to adapt their approach dynamically without technical expertise.
In community programs aimed at promoting social inclusion and engagement, practitioners can employ AI-enhanced tools to identify patterns in group interactions and preferences. For instance, community centers can use AI to analyze feedback from participants and adjust future programming to better meet the needs of diverse groups. This practical application can help public health initiatives build stronger, more connected communities and address social isolation effectively.
Policymakers could leverage these insights to advocate for integrating AI-enhanced psychosocial interventions within public health frameworks, leading to more cost-effective and scalable solutions. Additionally, educational institutions and training programs for therapists can include foundational AI literacy in their curricula to equip future practitioners with the skills to utilize these tools confidently. Technology developers can draw from this research to create specialized AI tools that align with the needs of non-technical users, ensuring their practicality and accessibility in both clinical and community-based art therapy settings.
Research limitations and future research opportunities
This study is not without limitations. The sample size, while sufficient for detecting significant effects, was relatively modest and limited to university students in a specific geographic region. This homogeneity may affect the generalizability of the findings to broader and more varied populations. Future research should involve larger, more diverse samples across different cultural and socioeconomic backgrounds to assess whether personalized AI-enhanced art therapy yields similar outcomes globally. Cultural variations, including differing attitudes toward technology and therapeutic practices, may influence the efficacy and acceptance of AI-driven interventions, impacting the generalizability of the results.
The reliance on self-reported measures for social connectedness and community engagement introduces potential biases related to participant self-perception and social desirability. To address this limitation, future studies could incorporate objective measures, such as third-party observations, digital interaction tracking, or biometric data (e.g., heart rate variability as an indicator of emotional response), to supplement self-reported data and provide a more comprehensive analysis of outcomes. This multimodal approach would help mitigate self-reporting biases and strengthen the validity of the findings.
The AI algorithms employed in this study, while effective, represent an initial implementation of personalization. Future research should explore the use of advanced machine learning models, such as adaptive learning algorithms and neural networks, which can evolve and fine-tune their recommendations based on more extensive data over time. The integration of real-time data processing with adaptive learning could offer more responsive customization, enhancing the effectiveness of art therapy sessions. Additionally, investigating the role of data fusion techniques that combine diverse data types (e.g., textual, behavioral, and physiological data) could further optimize therapy personalization and outcomes.
Challenges related to real-time feedback mechanisms and the practical implementation of AI tools suggest the need for improved infrastructure and technical support in future applications. Addressing these challenges could facilitate the scalability of AI-enhanced art therapy, making it more accessible and feasible for widespread adoption in clinical and community settings.
Future research should also examine the long-term impact of AI-enhanced personalized art therapy on social health metrics. While this study focused on an eight-week intervention period, understanding how sustained or periodic sessions influence long-term social connectedness, community engagement, and relationship satisfaction would provide valuable insights. Additionally, exploring the integration of AI-enhanced personalization with other psychosocial interventions, such as group therapy or cognitive-behavioral therapy, could expand the applicability of the findings and assess the comparative advantages of combined approaches.
Finally, this study underscores the importance of addressing ethical considerations when using AI in therapeutic settings. Future research should focus on issues related to data privacy, algorithmic transparency, and potential biases in AI-driven recommendations. Ensuring that these technological interventions are equitable and ethically sound is essential to fostering trust among practitioners and clients and promoting the responsible use of AI in mental health and psychosocial care.
Conclusion
This study demonstrates that AI-enhanced personalized art therapy significantly improves social connectedness, community engagement, and interpersonal relationship satisfaction compared to standardized art therapy and no intervention. By integrating AI with personalized medicine principles, this research highlights the potential for tailored psychosocial interventions to more effectively address individual needs. The findings contribute to advancing both theoretical and practical approaches within art therapy and precision medicine, underscoring the value of AI in augmenting adaptive and individualized therapeutic practices.
Declarations
The experiments conducted in this study have been pre-registered at https://osf.io/m6xrb/.
Ethical approval for the study was obtained from the Ethics Committee of Xi’an Jiaotong-Liverpool University (XJTLU), with the approval ID ER-LRR-11000027020240303235049.
This research was supported by the Teaching Development Fund (TDF2324-R28-237) and the Research Development Fund (RDF-23-01-016), both from Xi’an Jiaotong-Liverpool University.
References
- Heenan D. Art as therapy: An effective way of promoting positive mental health? Disability & Society. 2006; 21(2): 179-191. https://doi.org/10.1080/09687590500498143.
- Shukla A, Choudhari S, Gaidhane A, Quazi Syed Z. Role of art therapy in the promotion of mental health: A critical review. Cureus. 2022; 14. https://doi.org/10.7759/cureus.28026.
- Haeyen S, Chakhssi F, van Hooren S. Benefits of art therapy in people diagnosed with personality disorders: A quantitative survey. Frontiers in Psychology. 2020; 11. https://doi.org/10.3389/ fpsyg.2020.00686.
- Dilawari K, Tripathi N. Art therapy: A creative and expressive process. Indian Journal of Positive Psychology. 2014; 5(1): 81-85. https://doi.org/10.15614/IJPP/2014/V5I1/52948.
- Cheng L, Liu Y, Liu W. Precision medicine: From one size fits all to personalized healthcare. Frontiers in Genetics. 2021; 12: 694727. https://doi.org/10.3389/fgene.2021.694727.
- Hu J, Zhang J, Hu L, Yu H, Xu J. (2021). Art therapy: A complementary treatment for mental disorders. Frontiers in Psychology. 2021; 12. https://doi.org/10.3389/fpsyg.2021.686005.
- Johnson KB, Wei WQ, Weeraratne D, Frisse M, Misulis K, et al. Precision medicine, AI, and the future of personalized health care. Clinical and Translational Science. 2020; 14(1): 86-93.
- Filipp F. Opportunities for artificial intelligence in advancing precision medicine. Current Genetic Medicine Reports. 2019; 7(3): 208-213.
- Mehta V. Artificial intelligence in medicine: Revolutionizing healthcare for improved patient outcomes. Journal of Medical Research and Innovation. 2023.
- Su T, Wu CH, Kao J. Artificial intelligence in precision medicine in hepatology. Journal of Gastroenterology and Hepatology. 2021; 36(3): 569-580.
- Uttley L, Scope A, Stevenson M, Rawdin A, Taylor Buck E, et al. Systematic review and economic modelling of the clinical effectiveness and cost-effectiveness of art therapy among people with non-psychotic mental health disorders. Health Technology Assessment. 2015; 19(18): 1-120. https://doi.org/10.3310/ hta19180.
- Farokhi M. Art therapy in humanistic psychiatry. Procedia Social and Behavioral Sciences. 2011; 30: 2088-2092. https://doi. org/10.1016/J.SBSPRO.2011.10.406.
- Laranjeira C, Campos C, Bessa A, Neves G, Marques MI. Mental health recovery through art therapy: A pilot study in Portuguese acute inpatient setting. Issues in Mental Health Nursing. 2019; 40(5): 399-404. https://doi.org/10.1080/01612840.2018.1563255.
- Naik K, Goyal RK, Foschini L, Chak CW, Thielscher C, et al. Current status and future directions: The application of artificial intelligence/machine learning (AI/ML) for precision medicine. Clinical Pharmacology and Therapeutics. 2023.
- Mirnezami R, Nicholson J, Darzi A. Preparing for precision medicine. New England Journal of Medicine. 2012; 366(6): 489-491.
- Topol EJ. Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again. Basic Books. 2019.
- Vogenberg FR, Barash CI, Pursel M. Personalized medicine: Part 1: Evolution and development into theranostics. Pharmacy and Therapeutics. 2010; 35(10): 560-576.
- Jameson JL, Longo DL. Precision medicine-personalized, problematic, and promising. Obesity. 2015; 23(6): 1004-1011.
- Collins FS, Varmus H. A new initiative on precision medicine. New England Journal of Medicine. 2015; 372(9): 793-795. https://doi.org/10.1056/NEJMp1500523.
- Ashley EA. The precision medicine initiative: A new national effort. JAMA. 2016; 315(8): 793-794. https://doi.org/10.1001/ jama.2016.0297.
- Cheng P, Xu L, Zhang, J, Liu W, Zhu J. Role of arts therapy in patients with breast and gynecological cancers: A systematic review and meta-analysis. Journal of Palliative Medicine. 2021. https://doi.org/10.1089/jpm.2020.0468.
- Marini F, et al. Leveraging AI for adaptive therapy: Advancing psychosocial health through precision interventions. Healthcare Review. 2022; 18(2): 99-116.
- Esteva A, Robicquet A, Ramsundar B, Kuleshov V, DePristo M, et al. A guide to deep learning in healthcare. Nature Medicine. 2019; 25(1): 24-29.
- Joshi A, Mehta S, Pande N, Mehta A, Randhe K. Effect of Mindfulness-Based Art Therapy (MBAT) on psychological distress and spiritual wellbeing in breast cancer patients undergoing chemotherapy. Indian Journal of Palliative Care. 2021; 27: 552-560. https://doi.org/10.25259/ijpc_133_21.
- Obermeyer Z, Emanuel EJ. Predicting the future-big data, machine learning, and clinical medicine. New England Journal of Medicine. 2016; 375(13): 1216-1219.
- Lee RM, Robbins SB. Measuring belongingness: The Social Connectedness and the Social Assurance Scales. Journal of Counseling Psychology. 1995; 42(2): 232-241.
- Holt-Lunstad J, Robles TF, Sbarra DA. Advancing social connection as a public health priority in the United States. American Psychologist. 2017; 72(6): 517-530. https://doi.org/10.1037/ amp0000103.
- Haeyen S, van Hooren S, van der Veld W, Hutschemaekers G. Promoting emotional resilience through art therapy: A controlled trial. Frontiers in Psychology. 2020; 11: 571.
- Dilawari S, Tripathi R. Effectiveness of art therapy in treating trauma and emotional distress. Journal of Creative Therapies. 2014; 8(3): 45-57.
- Kapitan L. Introduction to art therapy research. Routledge. 2018.
- Putnam RD. Bowling alone: The collapse and revival of American community. Simon and Schuster. 2000.
- Kweon BS, Sullivan WC, Wiley AR. Green spaces and community health: Theoretical synthesis and practical applications. Community Health Journal. 2017; 42(2): 103-117. https://doi. org/10.1016/j.chj.2017.03.006.
- Marini F, Werner C, Dumouchel P. Personalized approaches in psychotherapy: A comprehensive review. Journal of Personalized Medicine. 2022; 12(5): 326. https://doi.org/10.3390/ jpm12050326.
- Attard A, Larkin M. Art therapy for people with psychosis: A narrative review of the literature. International Journal of Art Therapy. 2016; 21(3): 118-132. https://doi.org/10.1080/17454832.2016.1170059.
- Cox SM, Spooner A, Dunn M. Personalized medicine and public health: Ethical and social implications. Healthcare Ethics. 2021; 28(3): 245-258. https://doi.org/10.1080/13534528.2021.1860043.
- Joshi P, Smith J, Berman M. The role of AI in modern mental health treatment: Opportunities and challenges. Journal of Medical Systems. 2021; 45(6): 78. https://doi.org/10.1007/ s10916-021-01714-6.
- Fletcher GJO, Simpson JA, Thomas G. The measurement of perceived relationship quality components: A confirmatory factor analytic approach. Personality and Social Psychology Bulletin. 2000; 26(3): 340-354. https://doi.org/10.1177/0146167200265007.
- Haeyen S, van Hooren S, van der Veld W, Hutschemaekers G. Promoting mental health versus reducing mental illness in art therapy with patients with personality disorders: A quantitative study. Frontiers in Psychology. 2020; 11: 577020. https://doi. org/10.3389/fpsyg.2020.577020.
- Malchiodi CA. Creative interventions with traumatized children. Guilford Press. 2020.
- Goldberg D, Williams P. A User’s Guide to the General Health Questionnaire. NFER-Nelson. 1988.
- Jackson C. The General Health Questionnaire. Occupational Medicine. 2007; 57(1): 79-79. https://doi.org/10.1093/occmed/ kql169.
- Cohen S. Social relationships and health. American Psychologist. 2004; 59(8): 676-684. https://doi.org/10.1037/0003066X.59.8.676.
- Valtorta NK, Kanaan M, Gilbody S, Ronzi S, Hanratty B. Loneliness and social isolation as risk factors for coronary heart disease and stroke: Systematic review and meta-analysis of longitudinal observational studies. Heart. 2016; 102(13): 1009-1016. https://doi.org/10.1136/heartjnl-2015-308790.
- Patterson T, Heisel MJ, Holliday C. Enhancing participation in art therapy for older adults: A comprehensive approach. Journal of Art in Psychotherapy. 2011; 38(2): 110-119.
- Elkins DE, Deaver SP. The use of art in therapy: A survey of art therapists in various settings. Art Therapy: Journal of the American Art Therapy Association. 2015; 32(3): 121-129. https://doi. org/10.1080/07421656.2015.1060833.
- Malchiodi CA. The Art Therapy Sourcebook. McGraw-Hill Education. 2020.
- Joshi S, Kim W, Park J. The role of AI in enhancing psychotherapy: An exploration. Journal of Mental Health and Technology. 2021; 10(4): 211-223.